
The Big Knife incident....
Well, tomorrow is the big day for a little surgery. I have a pilonidal cyst that will be removed. Sadly this is the second time this has come up, and as luck would have it I have come down with a cold also.
Well, what is that weird crap you have, you may ask, I will let you read about it here.
It has since been established that pilonidal disease is an acquired condition involving midline pits in the natal cleft. These holes or pits are enlarged hair follicles in the skin. The nature of these distorted hair follicles is unclear. It has been suggested that gravity and motion of the gluteal folds create a vacuum that pulls on the follicle. Bacteria and debris enter this sterile area, producing local inflammation. Edema occludes the mouth of the follicle, which continues to expand, rupturing into the underlying fatty tissue. Keratin and pus escape, and a foreign body reaction results in a microabscess, which is similar to perforating folliculitis. The purulent material subsequently tracks within the presacral subcutaneous tissue, producing acute and chronic pilonidal abscesses, as well as potential laterally displaced and epithelialized tracts. The conversion from a microabscess to the burrowing infection defines pilonidal disease; the same forces that create the pits are thought to cause the conversion.
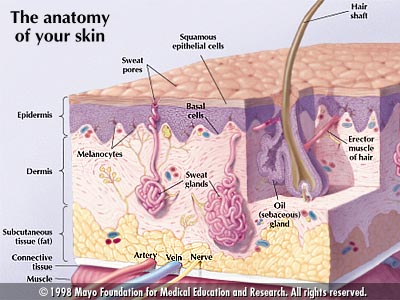
It was once thought that every pilonidal lesion contained a nest of hair. In reality, only 50% of cysts and sinuses are found to have hair during exploration. This finding, however, does not diminish its importance in the pathophysiology of pilonidal disease. Here is a link to a diagram of the epidermis http://www.jdenuno.com/epbimages/images/mayoskin.jpg
Hair has three distinct roles. The distended hair follicle plays the first role. It is not shed like its normal counterparts; it can remain in the follicle during its expansion. The hair contributes to local inflammation once the follicle ruptures, and it can even perforate the posterior wall of the follicle, enhancing microabscess formation. The second role is that of hairs from other parts of the body, which also can cause local disease. Free hairs act as secondary invaders, entering the follicle through its open mouth and contributing to the foreign body reaction. Neighboring hair in the skin surrounding pilonidal wounds plays the third role. These hairs act as mechanical irritators that affect wound healing. The second and third roles affect advanced pilonidal disease and maintain the adverse environment within the natal cleft.
Malignant degeneration rarely occurs in pilonidal disease, although verrucous carcinoma (giant condyloma acuminatum) has been described.
Here is a couple of links to what it looks like, if you are interested. I will warn you, this is of medical content, so it mught be a little gross looking to you.
This is the exit of the sinus , but it isn't of me, just a generic pic.
This is why I am glad they let you sleep during this.
Here is a pictoral site I found of the surgery.
I will be there at 5:30 a.m. and should be back home within 6 hours. Supposedly, I am to be off of work for one week, so my plan is do this on Fri. have Sta. And Sun. for recovery, and try and go back to work by Tuesday. I don’t like knowing that the workload is increased on my coworkers because of this, so I will try and get back as soon as I can, but I think I will be able to.
Hopefully I will put an update or two up while I am down and out.
Snappy
Well, what is that weird crap you have, you may ask, I will let you read about it here.
It has since been established that pilonidal disease is an acquired condition involving midline pits in the natal cleft. These holes or pits are enlarged hair follicles in the skin. The nature of these distorted hair follicles is unclear. It has been suggested that gravity and motion of the gluteal folds create a vacuum that pulls on the follicle. Bacteria and debris enter this sterile area, producing local inflammation. Edema occludes the mouth of the follicle, which continues to expand, rupturing into the underlying fatty tissue. Keratin and pus escape, and a foreign body reaction results in a microabscess, which is similar to perforating folliculitis. The purulent material subsequently tracks within the presacral subcutaneous tissue, producing acute and chronic pilonidal abscesses, as well as potential laterally displaced and epithelialized tracts. The conversion from a microabscess to the burrowing infection defines pilonidal disease; the same forces that create the pits are thought to cause the conversion.
It was once thought that every pilonidal lesion contained a nest of hair. In reality, only 50% of cysts and sinuses are found to have hair during exploration. This finding, however, does not diminish its importance in the pathophysiology of pilonidal disease. Here is a link to a diagram of the epidermis http://www.jdenuno.com/epbimages/images/mayoskin.jpg
{kind=link}
Hair has three distinct roles. The distended hair follicle plays the first role. It is not shed like its normal counterparts; it can remain in the follicle during its expansion. The hair contributes to local inflammation once the follicle ruptures, and it can even perforate the posterior wall of the follicle, enhancing microabscess formation. The second role is that of hairs from other parts of the body, which also can cause local disease. Free hairs act as secondary invaders, entering the follicle through its open mouth and contributing to the foreign body reaction. Neighboring hair in the skin surrounding pilonidal wounds plays the third role. These hairs act as mechanical irritators that affect wound healing. The second and third roles affect advanced pilonidal disease and maintain the adverse environment within the natal cleft.
Malignant degeneration rarely occurs in pilonidal disease, although verrucous carcinoma (giant condyloma acuminatum) has been described.
Here is a couple of links to what it looks like, if you are interested. I will warn you, this is of medical content, so it mught be a little gross looking to you.
This is the exit of the sinus , but it isn't of me, just a generic pic.
{kind=link}
This is why I am glad they let you sleep during this.
{kind=link}
Here is a pictoral site I found of the surgery.
{kind=link}
I will be there at 5:30 a.m. and should be back home within 6 hours. Supposedly, I am to be off of work for one week, so my plan is do this on Fri. have Sta. And Sun. for recovery, and try and go back to work by Tuesday. I don’t like knowing that the workload is increased on my coworkers because of this, so I will try and get back as soon as I can, but I think I will be able to.
Hopefully I will put an update or two up while I am down and out.
Snappy
posted by Snappy | 10/27/2005 06:54:00 PM
![]()
![]()
0 Comments:
Post a Comment
<< Home